AIMS:
Near-infrared spectroscopy (NIRS) detects lipid-rich coronary lesions with established predictive value for adverse cardiovascular events. Intensive lipid-lowering therapy including PCSK9 gene silencing is a promising approach to stabilize atherosclerotic plaque. Aim of this study was to assess the relationship between lipid content of analyzed coronary plaque and quantitative atherosclerosis regression parameters on the background of intensive lipid-lowering therapy including PCSK9 gene silencing.
METHODS AND RESULTS:
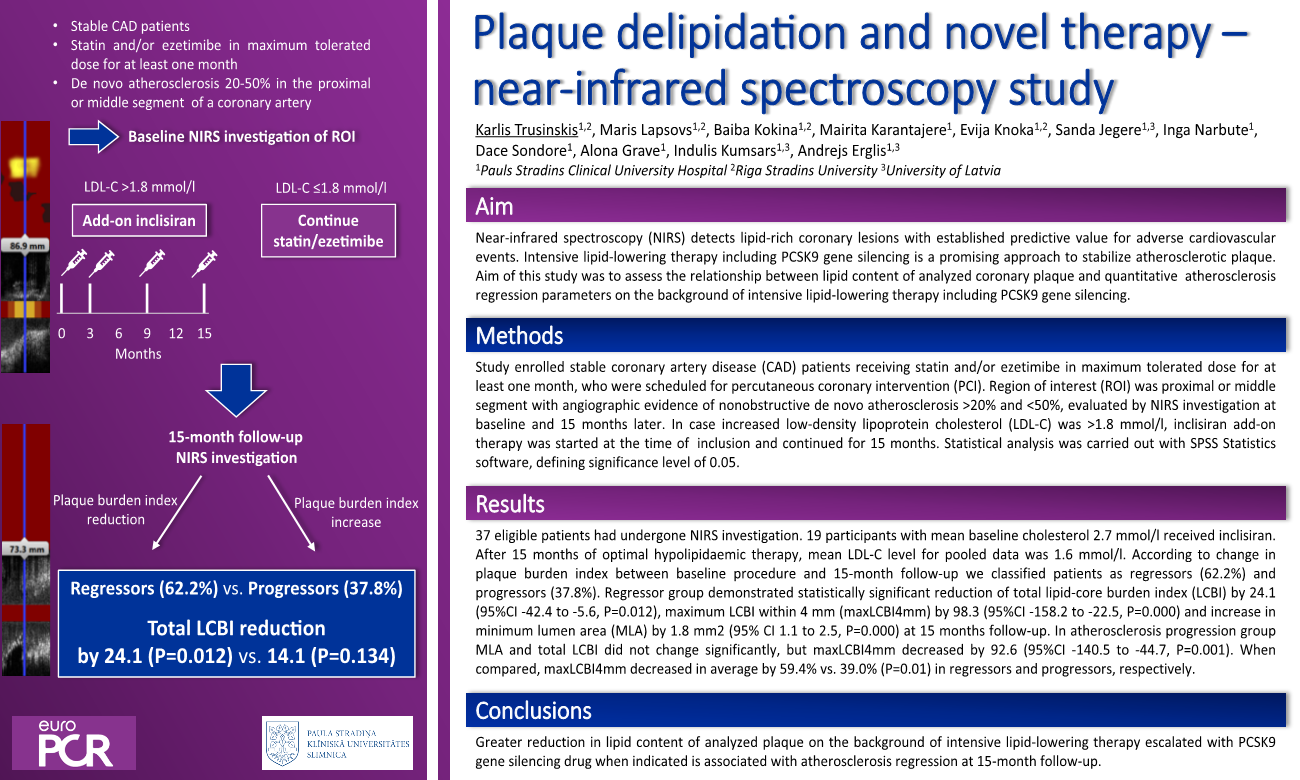
Study enrolled stable coronary artery disease patients receiving statin and/or ezetimibe in maximum tolerated dose for at least one month, who were scheduled for percutaneous coronary intervention (PCI). Region of interest was proximal or middle segment with angiographic evidence of nonobstructive de novo atherosclerosis >20% and <50%, evaluated by NIRS investigation at baseline and 15 months later. In case increased low-density lipoprotein cholesterol (LDL-C) was >1.8 mmol/l, inclisiran add-on therapy was started at the time of inclusion and continued for 15 months. Statistical analysis was carried out with SPSS Statistics software, defining significance level of 0.05. 37 eligible patients had undergone NIRS investigation. 19 participants with mean baseline cholesterol 2.7 mmol/l received inclisiran. After 15 months of optimal hypolipidaemic therapy, mean LDL-C level for pooled data was 1.6 mmol/l. According to change in plaque burden index between baseline procedure and 15-month follow-up we classified patients as regressors (62.2%) and progressors (37.8%). Regressor group demonstrated statistically significant reduction of total lipid-core burden index (LCBI) by 24.1 (95%CI -42.4 to -5.6, P=0.012), maximum LCBI within 4 mm (maxLCBI4mm) by 98.3 (95%CI -158.2 to -22.5, P=0.000) and increase in minimum lumen area (MLA) by 1.8 mm2 (95% CI 1.1 to 2.5, P=0.000) at 15 months follow-up. In atherosclerosis progression group MLA and total LCBI did not change significantly, but maxLCBI4mm decreased by 92.6 (95%CI -140.5 to -44.7, P=0.001). When compared, maxLCBI4mm decreased in average by 59.4% vs. 39.0% (P=0.01) in regressors and progressors, respectively.
CONCLUSION:
Greater reduction in lipid content of analyzed plaque on the background of intensive lipid-lowering therapy escalated with PCSK9 gene silencing drug when indicated is associated with atherosclerosis regression at 15-month follow-up.